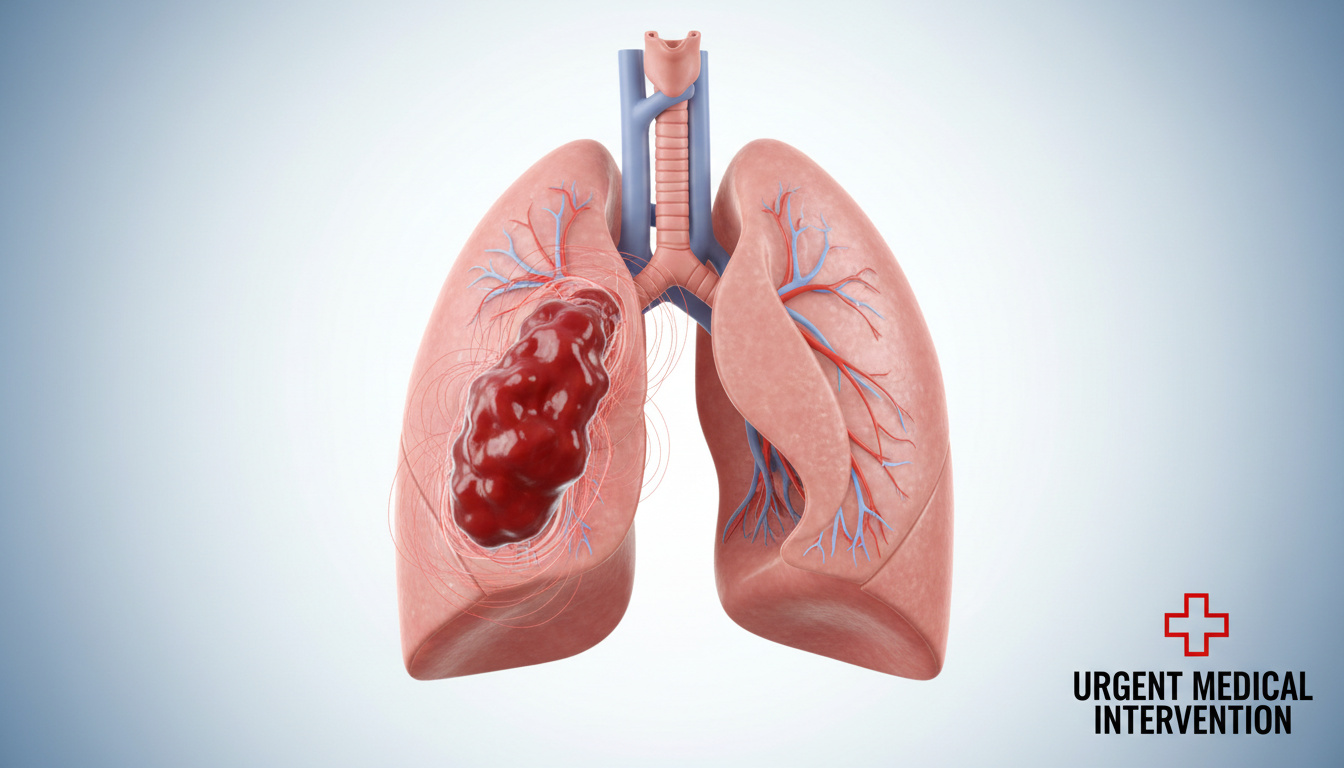
Pulmonary embolism occurs when a blood clot blocks an artery within the lung, most frequently originating as a deep vein thrombosis in the leg that migrates to the pulmonary circulation. This vascular occlusion constitutes a medical emergency capable of causing rapid cardiovascular collapse, though contemporary therapeutic protocols yield high survival rates when initiated without delay.
The condition announces itself through sudden physiological distress rather than gradual deterioration. Patients typically report acute respiratory compromise and thoracic pain that intensifies during inspiration. According to Harvard Health Publishing, the severity of presentation correlates directly with the volume of clot material obstructing pulmonary vessels and the patient’s underlying cardiopulmonary reserve.
Despite its lethal potential, pulmonary embolism responds to anticoagulant medications, thrombolytic agents, and supportive interventions. Diagnostic complexity persists, however, because symptom profiles frequently overlap with myocardial infarction, pneumonia, and anxiety disorders, complicating rapid identification in acute care settings.
What Are the Symptoms of a Blood Clot in the Lung?
Definition
Blockage in lung artery
Urgency
Life-threatening emergency
Common Source
Leg clots (DVT)
Key Stat
Often from deep vein thrombosis
- Symptoms typically begin suddenly rather than gradually
- Shortness of breath represents the most frequently reported symptom
- Chest pain often sharpens during deep breathing or coughing
- Presentation varies based on clot size and whether multiple clots exist
- Massive clots can cause fainting, bluish lips, or a sense of impending doom
- Leg pain or swelling may indicate the clot’s origin site
- Symptom overlap with cardiac and respiratory conditions complicates diagnosis
| Clinical Feature | Manifestation |
|---|---|
| Primary Respiratory Symptom | Sudden shortness of breath at rest or during activity |
| Pain Characteristics | Sharp chest pain worsening with inspiration or exertion |
| Cardiovascular Signs | Rapid or irregular heartbeat, palpitations |
| Respiratory Sounds | Wheezing, rapid breathing |
| Cough Presentation | Dry or productive of bloody mucus |
| Systemic Symptoms | Lightheadedness, dizziness, anxiety, excessive sweating |
| Cutaneous Indicators | Pale, clammy, or bluish skin discoloration |
| Source Indicators | Leg pain or swelling from associated DVT |
| Severity Markers | Fainting, bluish lips or fingernails |
The clinical presentation depends heavily on the burden of clot material within the pulmonary arteries. Harvard Health Publishing notes that smaller clots may produce subtle symptoms, while larger or multiple clots—such as saddle embolisms blocking major vessels—generate severe cardiopulmonary distress including syncope and cyanosis.
Peripheral indicators of the underlying thrombotic source frequently accompany pulmonary manifestations. Mayo Clinic specialists emphasize that leg swelling, pain, or tenderness indicates the presence of deep vein thrombosis, though these peripheral signs occasionally remain absent despite significant embolic burden.
What Causes a Blood Clot in the Lung?
Pulmonary embolism arises almost exclusively from dislodged thrombi originating in the deep venous system of the lower extremities. Cleveland Clinic specialists explain that when a clot formed in the leg breaks free, it travels through the venous return, passes through the right cardiac chambers, and lodges within the pulmonary arterial tree, obstructing perfusion to lung segments.
Deep Vein Thrombosis Connection
Deep vein thrombosis represents the precursor event for the vast majority of pulmonary emboli. Thrombus formation typically results from venous stasis, endothelial injury, or hypercoagulable states. Prolonged immobility—whether from surgical recovery, long-haul flights, or hospitalization—creates stagnant blood flow conducive to clot development in the deep leg veins.
The majority of pulmonary embolisms originate as deep vein thrombosis in the legs. Understanding leg symptoms proves crucial for early recognition, as treating the source DVT prevents further embolic events.
Risk Factors and Triggers
Multiple physiological and environmental factors increase clotting propensity. Research from Harvard Medical School identifies trauma, surgery, and inherited clotting disorders as primary catalysts. Hormonal changes, particularly those occurring during pregnancy or estrogen therapy, further elevate risk by altering coagulation dynamics and reducing venous return.
Pregnancy and Physiological Changes
Pregnancy significantly increases pulmonary embolism risk through multiple mechanisms. Venous compression from the enlarged uterus impedes blood return from the lower limbs, while hormonal fluctuations promote coagulation. According to Harvard Health, pulmonary embolism ranks among the leading causes of maternal mortality, necessitating heightened vigilance during gestation and the postpartum period.
How Is a Blood Clot in the Lung Treated?
Treatment protocols demand immediate hospitalization for hemodynamic monitoring and therapeutic intervention. Tampa General Hospital clinicians emphasize that therapeutic goals center on preventing clot propagation, dissolving existing thrombi, and averting recurrence through pharmacological management.
Anticoagulant Therapy
Blood thinners constitute the foundation of pulmonary embolism management. Initial treatment typically involves injectable heparin administered intravenously or subcutaneously, followed by transition to oral agents. Direct oral anticoagulants—including apixaban, rivaroxaban, dabigatran, and edoxaban—now serve as alternatives to traditional warfarin therapy, offering predictable dosing without routine coagulation monitoring.
Initial anticoagulant injections continue for at least five days alongside oral therapy. Treatment duration typically extends three to six months, though some patients require lifelong anticoagulation depending on recurrence risk and underlying conditions.
Thrombolytic Intervention
For massive pulmonary embolism accompanied by hypotension or cardiovascular collapse, thrombolytic agents provide rapid clot dissolution. Cedars-Sinai Medical Center notes that tissue plasminogen activator administered intravenously or via catheter-directed delivery carries elevated bleeding risk but proves life-saving in hemodynamically unstable patients.
Surgical and Procedural Options
Surgical embolectomy or catheter-based clot removal may become necessary when pharmacological therapy contraindicates or fails. These interventions typically reserve for severe cases where clot burden threatens immediate cardiovascular collapse.
Hospitalization duration varies by severity. Cleveland Clinic documentation indicates that while some patients with minor emboli may receive outpatient management, severe cases requiring ICU admission demand extended monitoring until hemodynamic stability returns.
What Is the Recovery Time for Blood Clots in the Lungs?
Recovery trajectories vary substantially based on embolism severity, patient comorbidities, and treatment response. Cleveland Clinic specialists report that many patients experience symptomatic improvement within one week of initiating anticoagulant therapy, though complete physiological resolution often requires months.
Short-Term Recovery
During the initial weeks, patients gradually regain pulmonary function as the body dissolves the clot through natural fibrinolytic processes. Anticoagulant medications prevent new clot formation while the vascular system recanalizes obstructed vessels. Activity tolerance typically improves within days to weeks, though residual fatigue may persist.
Long-Term Prognosis and Medication
Anticoagulation therapy generally continues for a minimum of three to six months to prevent recurrence. Some patients—particularly those with recurrent emboli or permanent risk factors—require indefinite anticoagulation. Tampa General Hospital notes that prolonged therapy decisions depend on balancing thrombosis risk against bleeding complications.
Survival and Complications
Prompt treatment dramatically reduces mortality. However, delayed or inadequate therapy permits progression to chronic thromboembolic pulmonary hypertension or right heart failure. The American Lung Association warns that recurrent embolism increases the risk of permanent pulmonary vascular damage, underscoring the importance of adherence to prophylactic regimens.
Smaller, isolated clots generally carry better prognoses than multiple or large saddle emboli. Massive pulmonary embolism can cause permanent heart and lung damage without immediate intervention.
What About Blood Clots in the Lung During Pregnancy or Multiple Clots?
Certain clinical scenarios demand specialized management protocols. Pregnancy-associated pulmonary embolism presents unique diagnostic and therapeutic challenges, while multiple simultaneous clots—particularly saddle emboli—constitute critical emergencies requiring aggressive intervention.
Pregnancy-Specific Considerations
Gestational pulmonary embolism requires careful medication selection to protect fetal development. Harvard Health Publishing confirms that while pregnancy significantly elevates risk, specific management protocols continue beyond the scope of current documentation, necessitating specialist consultation for therapeutic planning.
Multiple Clots and Massive PE
Saddle emboli—so named for their position straddling the pulmonary artery bifurcation—obstruct blood flow to both lungs simultaneously. These presentations generate severe hypoxia, cardiovascular collapse, and syncope. Such cases require immediate thrombolytic therapy or surgical intervention, with management occurring exclusively in intensive care settings.
How Does a Blood Clot in the Lung Progress Over Time?
Understanding the temporal sequence of pulmonary embolism aids in recognizing critical intervention windows. The pathophysiological course typically follows a predictable pattern from initial thrombosis through clinical resolution.
- Deep Vein Thrombosis Formation: Blood clots form in deep leg veins due to immobility, trauma, or hypercoagulable states, often developing over hours to days.
- Embolization: The thrombus detaches from the venous wall and travels through the inferior vena cava, right heart chambers, and into the pulmonary arterial system.
- Pulmonary Arterial Obstruction: The clot lodges in pulmonary vessels, causing ventilation-perfusion mismatch and hemodynamic compromise within minutes to hours.
- Symptom Onset: Acute dyspnea, pleuritic chest pain, and tachycardia manifest suddenly as lung tissue becomes ischemic.
- Immediate Treatment Window: Critical care intervention must begin within hours to prevent right ventricular failure and cardiovascular collapse.
- Resolution Phase: Over weeks to months, anticoagulation prevents extension while endogenous fibrinolysis dissolves the clot and restores perfusion.
What Is Established vs. What Remains Uncertain?
Medical consensus exists regarding many aspects of pulmonary embolism pathophysiology and treatment, though individual prognosis involves variables that resist precise prediction.
| Established Facts | Uncertain or Variable Factors |
|---|---|
| PE originates from DVT in the majority of cases | Exact survival timelines for untreated massive PE vary by patient age and comorbidity |
| Anticoagulants reduce mortality and recurrence | Specific duration of anticoagulation for individual risk profiles requires clinical judgment |
| Symptoms include sudden dyspnea and pleuritic pain | Precise incidence rates of misdiagnosis in specific populations remain understudied |
| Thrombolytics benefit hemodynamically unstable patients | Long-term psychological outcomes following PE recovery lack extensive documentation |
| Pregnancy significantly increases PE risk | Optimal screening protocols for asymptomatic postpartum thrombosis remain debated |
Why Is Pulmonary Embolism Frequently Misdiagnosed?
Diagnostic errors complicate pulmonary embolism management because presenting symptoms overlap multiple common conditions. The acute chest pain and dyspnea mimic myocardial infarction, while fever and cough may suggest pneumonia. Cedars-Sinai Medical Center acknowledges that this symptomatic ambiguity frequently delays appropriate treatment, particularly when patients lack obvious leg symptoms indicating DVT.
Anxiety and panic disorders further complicate differential diagnosis, as hyperventilation and chest tightness characterize both conditions. While Flu symptoms and relief typically involve gradual onset with fever and myalgias, and viral illnesses present with distinct patterns described in COVID symptoms and recovery, pulmonary embolism manifests abruptly without prodromal illness. This distinction proves critical for emergency triage.
What Do Leading Medical Institutions Say?
Pulmonary embolism is a blockage of a lung artery, usually by a blood clot that travels from a deep vein thrombosis (DVT) in the legs… It is life-threatening but treatable with anticoagulants, thrombolytics for severe cases, and supportive care.
Harvard Health Publishing
Pulmonary embolism is often difficult to diagnose because the symptoms overlap with heart attack, pneumonia, or anxiety.
Cedars-Sinai Medical Center
Quick treatment greatly reduces death risk… untreated massive PE can cause heart/lung damage or death.
Tampa General Hospital and Cleveland Clinic
What Are the Key Takeaways About Lung Blood Clots?
Pulmonary embolism represents a potentially fatal obstruction of pulmonary arteries, most commonly originating from deep vein thrombosis in the lower extremities. Sudden shortness of breath, sharp pleuritic chest pain, and tachycardia constitute the classic presentation, though symptom severity varies widely. Immediate anticoagulation therapy prevents clot propagation and reduces mortality, while recovery spans from days of symptomatic improvement to months of continued medication. Preventative measures, particularly for high-risk groups such as post-surgical patients and pregnant women, remain essential for reducing incidence.
Frequently Asked Questions
What are blood clot symptoms in the leg?
Deep vein thrombosis typically presents as unilateral leg pain, swelling, warmth, or tenderness. The affected limb may appear reddened or discolored compared to the unaffected side.
Can blood clots in lungs resolve on their own?
While the body naturally dissolves clots over time through fibrinolysis, pulmonary embolism requires medical treatment to prevent growth, additional clots, and fatal complications during the resolution process.
How is a blood clot in the lung different from a heart attack?
Pulmonary embolism causes sharp pain that worsens with breathing, while heart attack pain typically presents as crushing pressure unaffected by respiration. Both require emergency evaluation.
What is a saddle embolism?
A saddle embolism occurs when a large blood clot lodges at the bifurcation of the main pulmonary artery, blocking blood flow to both lungs simultaneously and causing severe cardiovascular collapse.
Are blood clots in the lungs always fatal?
Not with treatment. Prompt anticoagulation significantly reduces mortality risk. However, untreated massive pulmonary embolism carries high fatality rates due to right heart failure and circulatory collapse.
How long does anticoagulant treatment last?
Standard therapy continues three to six months for first-time events. Recurrent clots or permanent risk factors may necessitate lifelong anticoagulation to prevent future embolism.
Can you fly after having a blood clot in the lung?
Patients typically resume air travel after completing initial treatment and achieving stability, though they require clearance from their physician and may need compression stockings or prophylactic anticoagulation.
Oliver Jack Carter Cooper is a staff writer for EveningLedger.uk, covering UK news, politics, business and culture. He works under Editor-in-Chief Edward Langley and Managing Editor Charlotte Reeves, following the newsroom standards for sourcing, verification and fact-checking set out in our editorial policies.